
Disparities in Health
Why equitable care may lead to lower cost August/September 2018In 2017, tennis player Serena Williams won the Australian Open during the early stages of pregnancy and then gave birth to her first child later that year. The day after the cesarean birth, Williams experienced shortness of breath and recognized this as a symptom of pulmonary embolism (she has a history of embolisms). After a period of time spent trying to convince clinical staff that she needed immediate care, and a series of diagnostic tests, physicians eventually came to the same conclusion she had and gave her the necessary treatment for pulmonary embolism. However, Williams implied in a recent interview1 that she may have received necessary care more quickly if her claims had been taken seriously from the beginning. Even Williams, arguably one of the most powerful athletes to ever compete in any sport, struggled to make herself heard by medical practitioners, highlighting the fact that African-American women face significant disparities in the health care they receive during pregnancy and the postpartum period.
African-American women are three to four times more likely than white women to die from pregnancy-related causes.2 This phenomenon is consistent across income levels and ages. In addition, African-American infants in the United States are more than twice as likely to die as white infants, a wider disparity than in 1850 during the slavery era (when the United States began keeping records on infant mortality by race).3
In fact, disparities in health care—health differences that are closely linked with social, economic or environmental disadvantage4—exist based on race, gender, income, sexual orientation and spoken language, and exist across every medical condition and type of health care provider throughout the United States. Eliminating or even reducing such disparities in care would result in better health for all populations and would significantly reduce the cost burden of health care. Actuaries must recognize and understand health disparities and work to address the additional cost burden that disparities create.
DEFINING QUALITY AND ACCESS TO HEALTH CARE
The Institute of Medicine defines health care quality and access as follows:
- Quality is the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.
- Access to health care means having the timely use of personal health services to achieve the best health outcomes. Attaining good access to care requires three discrete steps:
- Gaining entry into the health care system
- Getting access to sites of care where patients can receive needed services
- Finding providers who meet the needs of individual patients and with whom patients can develop a relationship based on mutual communication and trust
Health Equity
According to the nonprofit health philanthropy Robert Wood Johnson Foundation, health equity means that everyone has a fair and just opportunity to be as healthy as possible.5 This requires removing obstacles to health such as poverty and discrimination; and removing their consequences, including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environments, and health care.
For the purposes of measurement, health equity means reducing and ultimately eliminating disparities in health and its determinants that adversely affect excluded or marginalized groups.
Elimination of disparities would help to give all people the same opportunity for good health and enable longer and improved lives. It would also help reduce the cost burden of health care in the United States: Nationally, health disparities totaled an estimated $102 billion in direct medical costs in 2016 and will cost an estimated $1.3 trillion from 2017 to 2022. Consumers bear an additional $28 billion in out-of-pocket costs each year because of health disparities.6,7,8
A Framework to Study Health Disparities
In order to understand the impact of health disparities on its members, the Clinical Research and Strategy team at customer-owned health insurer Health Care Service Corporation9 (HCSC) studied the excess costs attributed to negative outcomes for different ethnic, gender, language proficiency, urbanicity and income cohorts among its members. Specifically, we looked at the health care outcomes in general as well as specific conditions.
Figure 1 outlines three types of disparity drivers: disparities in health, disparities in health care, and social and environmental determinants of health.
Figure 1: Causes of Excess Costs Due to Health Disparities

Source: Health Care Service Corporation
Disparities in Health: Variations in Disease Prevalence and Cost
The first type of health disparity driver is observed from excess costs and excess disease prevalence across various cohorts and compared to overall population benchmarks. For example, in the national population, African-Americans under age 35 are five times more likely than the average American to die from asthma. Transgender or gender nonbinary people have significantly higher rates of mental health care utilization and higher emergency department utilization than their cis-gender counterparts.10 Transgender people are 10 times more likely to attempt suicide than the average population.
HOW THE HCSC DATA SET WAS DERIVED
The Health Care Service Corporation (HCSC) data set used in this article was derived from the following:
- Using claims data from the highest cost 10 major diagnostic categories (MDCs) for members aged 18–64, “excess” costs were quantified for each cohort (by ethnicity), within each diagnostic category.
- Excess costs were defined as average per-capita costs that exceeded either the median or minimum per-capita spend by cohort for the same MDC.
- Results were segmented by line of business (LOB) and year across all member-residing states.
- Analysis used data from the Latino Strategy Study, which was received from the Enterprise Analytics team in January 2017.
- Ethnicity for each claimant was imputed from Acxiom data; further analysis of primary source race, ethnicity and language data should be prioritized to verify findings—particularly for group members.
- Diseases not included in each cohort’s highest costing 10 MDCs are not included in this analysis; thus, the cost of disparities may be understated.
- Calculated paid medical cost per claimant (paid cost per claimant per MDC, per ethnic cohort, by LOB and year).
- Determined cohort with median and minimum paid cost per claimant for each MDC.
- Calculated the average excess cost per claimant per cohort, per MDC, against two benchmarks:
- Cohort with median paid cost per claim by MDC
- Cohort with minimum paid cost per claim by MDC
- Multiplied average of excess cost per claimant for MDC by the number of claimants per cohort for MDC.
- Summarized total cost of disparities by condition, cohort, LOB and state.
Within the HCSC population, several conditions drove excess medical costs due to disparities. Musculoskeletal conditions such as lower back pain resulted in an annual $1.2 billion of costs that could be avoided because of health disparities. Respiratory diseases such as asthma and chronic obstructive pulmonary disease (COPD) generated about $600 million of excess costs due to disparities. Other conditions with high excess costs include myeloproliferative diseases such as lymphoma and leukemia, liver diseases, and circulatory diseases such as hypertension and coronary artery disease (CAD).
Disparities in Health Care: Variations in Quality and Access
The second type of driver is health care disparities, which can be measured by variations in the delivery of health care associated with variables that can affect quality of, and access to, health care services.
Many studies document the disparities in health care quality and access for African-Americans.11 In comparison with their white American counterparts, and even accounting for factors such as insurance status, income, age, co-morbid conditions and symptom expression, African-Americans:
- Are less likely to receive appropriate cardiac medication.
- Are less likely to undergo coronary artery bypass surgery.
- Are more likely to be late-stage diagnosed for breast cancer.
- Are less likely to receive hemodialysis and kidney transplantation.
- Are more likely to receive a lower quality of basic clinical services such as intensive care.
- Have significantly higher rates of life-threatening pregnancy and childbirth complications.
The HCSC data analysis highlights three major interrelated factors that influence quality and access to care.
- Income. In general, income has a stronger relationship with total health costs than ethnicity. This fact may be especially important when thinking about benefit design and member cost sharing.
- Urbanicity. Urban residence correlates with emergency department (ED) use for nonemergent medical needs, possibly signaling low access to nonfacility outpatient services. Rural residence correlates with lower use of both ED and outpatient services. High crime and violence areas also reduce access to quality health care as well as increase stress levels of residents, which has been associated with negative health outcomes.
- English language proficiency. English language proficiency can have a significant effect on how early disease is detected and how effectively it is managed over time.
Social Determinants of Health
The concept of social determinants of health (SDOH) has received considerable attention from the public health and health care communities in recent years. Social determinants, such as a person’s environment or personal characteristics, make up the complex set of home and community factors that shapes every person’s life. They are sometimes referred to as the upstream drivers of health since they may seem very indirectly related to health and can occur many years before a health event or outcome.12
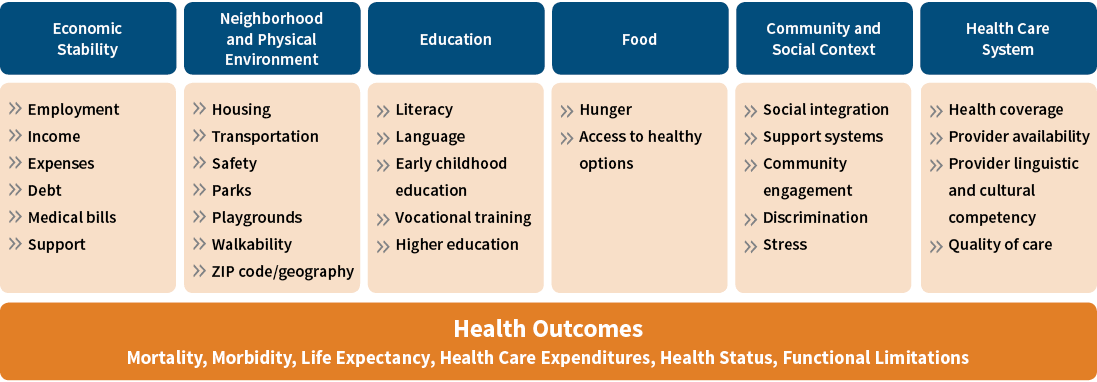
In the framework presented, SDOH is the underlying foundation, because if these upstream causes of poor health could be fully addressed, other disparities would be reduced significantly. For example, programs in Portland, Chicago and Minneapolis provide housing and other nonmedical social services to vulnerable populations and have reduced the cost of health care by up to 55 percent over several years.13 In this example, addressing the social determinant of stable housing can improve health and reduce health care costs. Figure 2 illustrates the many social determinants of health.
Figure 2: Social Determinants of Health
Click Image to Enlarge
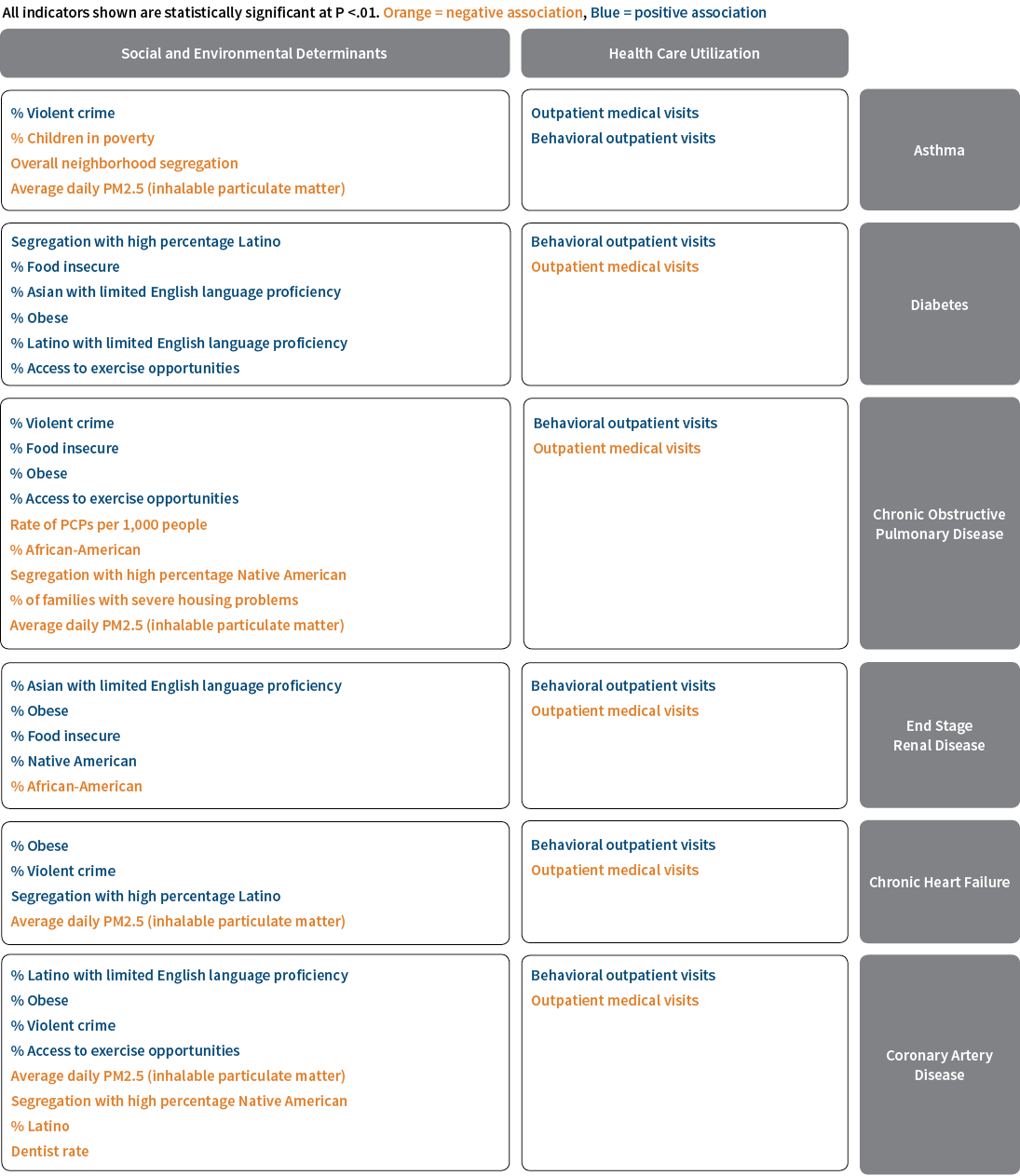
Based on publicly available data and HCSC data by ZIP code, the impact of several social and environmental determinants of health were analyzed by the HCSC Enterprise Analytics team to uncover statistically significant drivers of several high-cost health outcomes for HCSC’s employer group members. (See Figure 3.)
Figure 3: Statistically Significant Determinants of Health
Click Image to Enlarge
Source: Health Care Service Corporation
Not surprisingly, higher incidence of asthma is associated with PM2.5, a common measure of atmospheric particulate matter, or air quality. But asthma is also positively associated with the rate of violent crime. Such associations may also indicate a relationship between stress and asthma.
As might also be expected, diabetes incidence is associated with the obesity rate, food insecurity and access to exercise opportunity. However, it is also associated with lack of language proficiency, suggesting that diabetics may not be able to understand treatment options as described by clinicians who predominantly speak English.
Coronary artery disease (CAD) incidence is also associated with PM2.5, exercise opportunity and violent crime, but perhaps more surprisingly it is also associated with a lack of access to dentists. A recent article (see the Public Health web-exclusive series of The Actuary14) highlights the importance of dental care; poor dental care can lead to several serious medical conditions such as CAD, endocarditis and exacerbation of other diseases.
The Path Forward
A number of initiatives are successfully addressing disparities for vulnerable populations. Hennepin Health in Minnesota has developed an accountable care organization15 to address social determinants of health for the local Medicaid population. Through partnerships with behavioral health and housing organizations, it has improved care for members with chronic conditions, reduced utilization of emergency room visits and reduced overall health care costs.16
Since 2012, the state of Oregon has been working to transform its Medicaid program to encourage greater coordination of care and deliver care through regional coordinated care organizations (CCOs). (Oregon’s Medicaid transformation was described in the Public Health web-exclusive series of The Actuary earlier this year.17) Oregon’s CCOs were required to develop transformation plans to reduce disparities in care. The state also established health equity coalitions, which advise CCOs on cultural and linguistic diversity, and increased its investment in community health workers. These interventions were associated with a reduction over time in a narrowing of the disparity in primary care utilization, an important factor in disease prevention.18
These examples share a number of policy tools and strategies that are emerging to address the SDOH.19 Other strategies that programs may use to address disparities and improve a population’s health include:
- Use of health impact assessments to review needed, proposed and existing social policies for their likely impact on health.
- Application of a “health in all policies” strategy, which introduces improved health for all and the closing of health gaps as goals to be shared across all areas of government.
Actuaries must play a role in supporting policy changes that address social determinants and eliminate disparities. We can address health disparities with these actions:
- Support the collection of data by our employers, wherever possible, to include variables such as race, ethnicity, housing status, language and nonbinary gender identification. At the very least, merge neighborhood data such as those used in the HCSC study.
- Incorporate these variables into risk adjustment, pricing, valuation and forecasting work to show their importance.
- Analyze these variables and demonstrate the cost/benefit of investments in programs that address SDOH.
- Structure financial incentives for providers that address differences in care access and quality for marginalized members.
- Get involved with local public health and community organizations to bring an actuarial mindset to public health discussions.
Conclusion
It is financially and socially expedient to address health care inequities. According to the U.S. Census Bureau, in less than 25 years, half of the U.S. population will comprise people of color; we need to be prepared to care for an increasingly diverse population. By understanding health disparities and social determinants of health, we can improve health equity and reduce overall health spend.
References:
- 1. Haskell, Rob. 2018. “Serena Williams on Motherhood, Marriage, and Making Her Comeback.” Vogue. January 10. ↩
- 2. Centers for Disease Control and Prevention. 2018. “Pregnancy Mortality Surveillance System.” August 7. (accessed June 24, 2018). ↩
- 3. Villarosa, Linda. 2018. “Why America’s Black Mothers and Babies Are in a Life-or-Death Crisis.” The New York Times Magazine. April 11. ↩
- 4. Office of Disease Prevention and Health Promotion. 2018. HealthyPeople.gov. U.S. Department of Health and Human Services. (accessed June 24, 2018). ↩
- 5. Braveman, Paula, Elaine Arkin, Tracy Orleans, Dwayne Proctor, and Alonzo Plough. 2017. “What Is Health Equity? And What Difference Does a Definition Make?” Robert Wood Johnson Foundation. May. ↩
- 6. LaVeist, Thomas A., Darrell J. Gaskin, and Patrick Richard. 2009. “The Economic Burden of Health Inequalities in the United States.” Joint Center for Political and Economic Studies. September. ↩
- 7. Centers for Medicare and Medicaid Services. 2018. “NHE Fact Sheet.” April 17. (accessed July 17, 2018). ↩
- 8. National Urban League. 2012. “Health Disparities Cost U.S. Economy $82b in Higher Healthcare Spending and Lost Productivity.” December 5. ↩
- 9. Health Care Service Corporation operates Blue Cross Blue Shield plans in Illinois, Montana, New Mexico, Oklahoma and Texas. ↩
- 10. Progovac, Ana M., Benjamin Lê Cook, Brian O. Mullin, Alex McDowell, Maria Jose Sanchez R., Ye Wang, Timothy B. Creedon, and Mark A. Schuster. 2018. “Identifying Gender Minority Patients’ Health and Health Care Needs in Administrative Claims Data.” Health Affairs 37 (3). ↩
- 11. Smedley, Brian D., Adrienne Y. Stith, and Alan R. Nelson, eds. 2003. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, D.C.: National Academies Press. ↩
- 12. Freedman, David H. 2018. “Health Care’s ‘Upstream’ Conundrum.” Politico. January 10. ↩
- 13. Ibid. ↩
- 14. Sayre, Shereen. 2018. “Eliminating the Medical/Dental Care Divide.” The Actuary. February. ↩
- 15. According to the Centers for Medicare and Medicaid Services (CMS), an accountable care organization (ACO) is defined as a group of doctors, hospitals and other health care providers who come together voluntarily to give coordinated, high-quality care to their patients. ↩
- 16. Sandberg, Shana F., Clese Erikson, Ross Owen, Katherine D. Vickery, Scott T. Shimotsu, Mark Linzer, Nancy A. Garrett, Kimry A. Johnsrud, Dana M. Soderlund, and Jennifer DeCubellis. 2014. “Hennepin Health: A Safety-net Accountable Care Organization for the Expanded Medicaid Population.” Health Affairs 33 (11): 1975–1984. ↩
- 17. Shenoy, Sudha, and Michelle Mickey Rork. 2018. “Oregon Medicaid Transformation.” The Actuary. February. ↩
- 18. McConnell, K. John, Christina J. Charlesworth, Thomas H. A. Meath, Rani M. George, and Hyunjee Kim. 2018. “Oregon’s Emphasis on Equity Shows Signs of Early Success for Black and American Indian Medicaid Enrollees.” Health Affairs 37 (3). ↩
- 19. Office of Disease Prevention and Health Promotion. “Social Determinants of Health.” U.S. Department of Health and Human Services. (accessed June 24, 2018). ↩
Copyright © 2018 by the Society of Actuaries, Schaumburg, Illinois.