
Participatory Risk Management
Lessons for adaptation in the health sector
July 2020Photo: istock.com/vicnt
As the world grapples with its response to the COVID-19 pandemic, optimizing the allocation of limited resources is on the mind of policymakers. Moreover, the ensuing recovery effort will need to similarly determine how to plan for similar responses in txhe future. This includes the extent to which investment should be allocated to anticipatory or preemptive arrangements on the one hand, or to contingent arrangements that would be invoked only following the advent of a pandemic on the other.
Similar optimization approaches also are needed in the context of responding to the risks of climate change. In particular, policymakers should address the balance between investing in preemptive measures and in reactive or contingent measures, and determine cases where loss acceptance might be even more prudent.
One helpful approach that can be applied to the case of climate change impacts, as well as to that of health risks (including pandemics), is a preemptive adaptation, contingent arrangements and loss acceptance (PCL) framework.1
The PCL Framework—A Strategic Approach to Comprehensive Risk Management
Following a typical hydrometeorological disaster, a layman might read media reports that, of the magnitude of the total loss, only a certain percentage was insured. Therefore, they would conclude that one should maximize insurance coverage. Yet, in other contexts, people hear that each dollar of preventive action saves $7 or more in reactive costs, implying that one should maximize preemptive risk reduction.
This begs the question: How do we optimize the balance between different paths of risk management in the context of climate change? Existing methodologies for risk layering do not provide an answer to how to determine that threshold. To complicate things further, climate change practitioners recognize that reaching the “state of being adapted” or “resilient” to climate change is not just a numbers game and a factual or formulaic exercise. Rather, it is partly premised on cultural and societal values, which makes such assessments quite complicated.
Climate-related losses in recent years frequently have exceeded estimates, which often has strained the ability of national systems to respond to such eventualities adequately. The same can be said of other nonclimate-related events like the COVID-19 pandemic. Such events have increasingly strained government capacities in serving as “insurers of last resort.” This notion has held true in both developed and developing countries, and has revealed a gap in existing climate risk management approaches in averting loss of life and human suffering, and in minimizing destruction and loss of assets.
In the context of climate change, practitioners typically prioritize risk-reduction measures for events that are characterized by low severity and high frequency, and they prioritize insurance and contingent finance measures for events that are characterized by higher severity and lower frequency. Those with the highest severity are left to unplanned response and typically are addressed through emergency ad-hoc support systems that aid humanitarian response and relief operations.
Therefore, under current practice for climate change response, preemptive action is implied to be the most desirable type of response, followed by contingent action, followed by humanitarian or similar interventions to address whatever losses are left over from the climate impacts under consideration. But this implicit hierarchy can be inconsistent with the need to evolve toward comprehensive approaches that take into account all possible responses. Such adaptive responses should include loss acceptance where this is most appropriate, and they should take account of societal values and optimize the range of possible responses, consistent with these societal values, in addition to economic considerations.
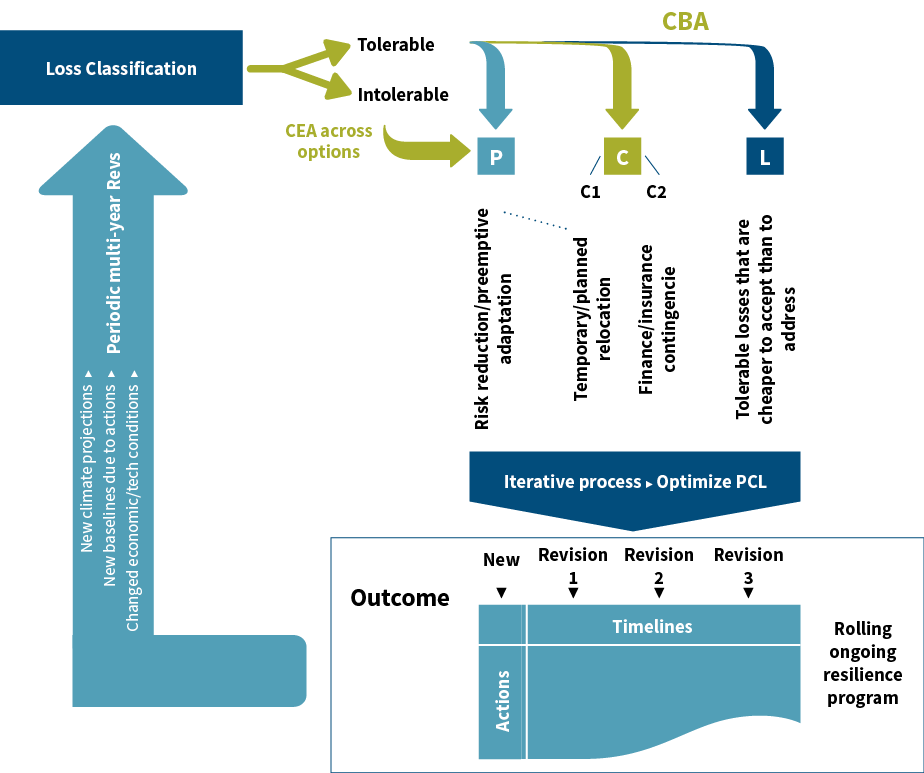
The PCL methodology is an approach to respond to this need. The process is illustrated in Figure 1.
Figure 1: The PCL Cycle
The current timing for this approach is opportune, considering recent advances in risk quantification, with the use of quantitative predictive models; geographic information systems and remotely sensed data; and the future prospects promised by big data analytics, the resurgence of artificial intelligence (AI) and the emergence of the Internet of Things (IoT). These technologies are starting to give direction to the value of adopting a rigorous (stepwise) approach for optimizing comprehensive risk management, and they present opportunities for reducing information asymmetries and for using predictive analytics in new ways that can reduce the total cost of adaptation.
The PCL framework presents a systematic approach to address these new realities and goes beyond existing efforts in a way that is relevant to both climate change planning and policy. It calls for optimizing response across three main response clusters with no predetermined hierarchy:
- Preemptive adaptation (P) or risk reduction
- Contingent arrangements (C)
- Loss acceptance (L)
This “framework” includes the three clusters of resource outlay on a single continuum. So, the outcome would be a balanced portfolio of actions across these three clusters by way of an optimization exercise. The approach would be applied separately for each hazard to which the target community is exposed.
The first step of this approach is an assessment of loss tolerability—a value-driven consultative assessment by society in which it determines which losses it considers to be tolerable and which ones are intolerable. Each of these two sets of loss categories undergoes a different assessment path that ensures the resulting optimization of actions across all losses is centered on a social valuation that is not limited to economics, but rather incorporates the real value of losses as determined by the stakeholders. The benefit of this is that the approach will enjoy societal buy-in, as it is fully consistent with the community’s valuation of loss tolerance—it gives that community a strong voice in the risk management decisions of their elected officials.
The response to intolerable losses is addressed exclusively through the “preemptive” action category. This step entails assessing risk reduction action to eliminate intolerable losses. The results of the first step, therefore, serve as input to the second step on contingent arrangements. The intolerability of the losses under consideration in the first step means that action should be taken to minimize their risk, even if the direct financial benefits outweigh the costs.
Finally, the third segment of the optimization spectrum is that of loss acceptance. This applies in cases where the societally assessed cost of loss is less than that of preemptive or contingent action. This largely overlaps with the concept of “risk retention.”
The PCL methodology also builds on synergy across the three response clusters. Assessment iterations are applied to reach fully optimized resource outlays across the P, C and L clusters. In conducting cost-benefit analysis for decision-making on tolerable losses, this applies for the financial, economic and social components of the actions under consideration. This will help consider the costs and benefits to affected demographics beyond the geographic region directly impacted. It also hopefully will prevent the selected actions from leading to an exacerbation of inequalities and inequities.
A wider, iterative and multiyear cycle also is envisaged. This addresses macro-level changes in climate projections, risk quantification, and societal perceptions and values, readjusting or fine-tuning previously prioritized action in light of such changes.
Lessons for Adaptation in the Health Sector
In applying the PCL framework to the health sector, a number of special considerations emerge.
Preemptive measures designed to eliminate intolerable loss, namely loss of life. These are measures that lead to increased capacity and resilience of the health system. They also take into account preparedness for less likely scenarios and the situations of vulnerable people.
According to the World Bank, depending on the severity of a pandemic, for example, economic losses can range from 0.5 percent to 4.8 percent of global gross domestic product (GDP). A 2013 World Bank paper estimated that in a severe pandemic scenario like the 1918 flu pandemic (when between 50 million and 100 million people in a global population of less than 2 billion died), economic losses could amount to 4.8 percent of global GDP, or more than $3 trillion. A moderate flu pandemic could have an impact of about half of this magnitude, and weak pandemics, such as the 2009 H1N1 flu pandemic, may result in economic impacts of less than 0.5 percent of GDP.2
This is similar to other high-priority threats like climate change. It is estimated that between 2030 and 2050, climate change will cause approximately 250,000 additional deaths per year from malnutrition, malaria, diarrhea and heat stress. The Intergovernmental Panel on Climate Change (IPCC) reported that climate change may extend some infectious diseases into places that are currently unaffected. Some climate-sensitive infectious diseases like dengue, with more than 90 million symptomatic cases per year, represent a particularly significant global disease burden.
Additionally, extreme weather events disrupt infrastructure critical to maintaining access to health care and emergency services. Tropical cyclone Harold, for example, resulted in loss of life and destruction in Vanuatu, Fiji, the Solomon Islands and Tonga at the same time these governments were working hard to contain the spread of the COVID-19—worsening the existing vulnerabilities of the countries.
Under the PCL approach, the risk of loss of life should be reduced to zero through the use of preparedness and preemptive action. Such preemptive action, especially in reducing climate-induced health risk, is a global public good. Strong health systems that effectively reach all people—especially the most vulnerable—are the only way to ensure protection from major disease outbreaks. Because a strong health system minimizes the potential for such outbreaks to spread beyond borders, it is a global benefit.
Additional measures, such as planned relocation, for example, are other avenues that can be used to minimize intolerable risks as much as possible. Under the PCL framework, cost-effectiveness analysis—rather than cost-benefit analysis—is employed to select the appropriate response. This is due to the fact that attaining the risk minimization goal for intolerable losses is a sine qua non, and attaining a positive net present value would not be the main criterion for proceeding with response measures. Rather, selecting the most cost-effective of different alternatives to achieve said minimization, even if all options under consideration exhibit costs that are higher than their associated financial and economic benefits, would be the goal.
Contingency plans. These are the inseparable pillar of comprehensive risk management for the health sector to respond to threats of climate change. The plans are invoked when the impact materializes and include mechanisms like insurance as well as other arrangements such as disaster-based hospitals, which are responsible for supporting other hospitals by accepting patients and dispatching medical personnel during a disaster.
Health care management during extreme weather events, emergencies and crises is the most vital part of contingent disaster management and response. Climate change is expected to exacerbate current systems by affecting health care access and delivery and widening inequalities in access to health services.
According to a 2015 report by the World Health Organization (WHO) and the World Bank, at least 400 million people do not have access to essential health services. Also, the report showed that across 37 countries, 6 percent of the population was falling back into extreme poverty (living on $1.25/day) due to the health cost they had to pay out of their own pockets.3 In the United States, despite historical progress in health insurance coverage, approximately 27 million nonelderly Americans were reported to be uninsured in 2016. The most uninsured people are among low-income families and people of color, who are at a higher risk of being uninsured than non-Hispanic whites.4
Additionally, there are many examples around the world of health care delivery challenges during extreme weather events, which highlights the importance of contingency plans. For example, one study that took account of future climate projections for flood risk to health care assets in the United Kingdom reported that the “proportion of care homes, emergency services, hospitals and doctors’ surgeries at risk of flooding in England is set to increase by 13 percent, 11 percent, 4 percent and 12 percent, respectively, by the 2050s under a 2-degree [Celsius] warming scenario.”5
Another study on power outages, extreme events and health identified 52 power outages across 19 countries that occurred as a direct result of extreme events.6 This is while electricity has been recognized as the most vital infrastructure for health care by some countries (e.g., the United Kingdom and Japan), because without it, most health services cannot function.
With an increasing trend for people with functional needs—such as people with respiratory illnesses needing respirators across the world—and an increase in the intensity and frequency of extreme weather events, the health sector is becoming more vulnerable to the threats of climate change. In response, some have suggested relocating hospitals to low-risk areas, or having more than one regional electrical provider.7 Japan has developed extensive contingency measures after experiencing severe earthquakes, including issuing a core plan of emergency care system reinforcement at disasters in 1996 and requirement criteria for the disaster-based hospitals.8 A survey in 2012 showed that 653 hospitals had been appointed as disaster-based hospitals in Japan.9 The PCL framework stresses the importance of the comprehensive assessment of all contingency options, using cost-benefit analysis to inform the selection of optimal ones.
Acceptable loss. Climate change-induced heat stress is predicted to lead to productivity loss amounting to 80 million jobs.10 Accepted losses in this regard would be those productivity losses that lie within a range that avoids long-term harm to well-being and cannot be addressed through preemptive and contingency plans. Another example of acceptable loss is how most people have embraced social distancing and loss of opportunity for leisure to prevent the spread of COVID-19.
The iterative aspect of the approach. This takes into account changing factors like societal priorities, technological advances, economic realities or new data as they become available, such as climate projections and changes in demographic data. The transforming demographic trend of population aging is considered to be one of the greatest future challenges for national health systems. The number of people over age 65 is expected to increase globally from 1 in 11 in 2019 to 1 in 6 by 2050, with most of the increase taking place in developing countries.
Additionally, numerous studies on vulnerability to climate change have shown that elderly people are one of the most vulnerable groups. The upward shift in the age distribution of the population—and the rising burden of age-related disability and co-morbidities accompanying population aging and, therefore, care demands—will put tremendous pressure on health and economic systems. They also pose substantial societal challenges that will result in increased future vulnerabilities to climate change; hence the need to feed these data into the optimization process periodically.
Conclusion
Response optimization using PCL varies considerably across countries due to several factors, including variances in climate hazards and risk, and differences in capacity of national health systems and in national health expenditure per capita. According to the World Bank data in 2017, total health expenditure per capita was US$10,246.14 for the United States and US$37.33 for the Democratic Republic of the Congo. Nonetheless, even in developed countries, the allocation of resources and losses is not yet optimized. This implies that, given the IPCC predicted with high confidence an increase in climate-related risks for natural and human systems due to warming of 1.5 degrees Celsius, current arrangements will be even more inadequate, and the need for finding the most effective balance of responses to climate risk will be even more pressing.
The views expressed in this article are those of the authors, and do not necessarily represent the view of the United Nations Framework Convention on Climate Change.
References:
- 1. Nassef, Youssef. The PCL Framework: A Strategic Approach to Comprehensive Risk Management in Response to Climate Change Impacts. Cornell University, April 13, 2020 (accessed June 15, 2020). ↩
- 2. Jonas, Olga B. Pandemic Risk. The World Bank, 2013 (accessed May 27, 2020) ↩
- 3. World Health Organization and The World Bank. Tracking Universal Health Coverage: First Global Monitoring Report. World Health Organization, 2015 (accessed May 27, 2020). ↩
- 4. Tolbert, Jennifer, Kendal Orgera, Natalie Singer, and Anthony Damico. Key Facts About the Uninsured Population. Kaiser Family Foundation, December 13, 2019 (accessed May 27, 2020). ↩
- 5. Landeg, Owen, Geoff Whitman, Kate Walker-Springett, Catherine Butler, Angie Bone, and Sari Kovats. 2019. Coastal Flooding and Frontline Health Care Services: Challenges for Flood Risk Resilience in the English Health Care System. Journal of Health Services Research & Policy 24, no. 4:219–228. ↩
- 6. Klinger, Chaamala, Owen Landeg, and Virginia Murray. 2014. Power Outages, Extreme Events and Health: A Systematic Review of the Literature From 2011–2012. PLoS Currents 6. ↩
- 7. Supra note 5. ↩
- 8. Homma, Masato. 2015. Development of the Japanese National Disaster Medical System and Experiences During the Great East Japan Earthquake. Yonago Acta Medica no. 2:53. ↩
- 9. Kudo, Daisuke, Hajime Furukawa, Atsuhiro Nakagawa, Satoshi Yamanouchi, Yuichi Koido, Takashi Matsumura, Yoshiko Abe, et al. 2013. Resources for Business Continuity in Disaster-based Hospitals in the Great East Japan Earthquake: Survey of Miyagi Prefecture Disaster Base Hospitals and the Prefectural Disaster Medicine Headquarters. Disaster Medicine and Public Health Preparedness 7, no. 5:461–466. ↩
- 10. International Labour Organization. Working on a Warmer Planet: The Impact of Heat Stress on Labour Productivity and Decent Work. International Labour Organization, 2019 (accessed June 17, 2020). ↩
Copyright © 2020 by the Society of Actuaries, Chicago, Illinois.